Arq. Bras. Cardiol. 2021; 117(1): 15-25
Accuracy of Post-thrombolysis ST-segment Reduction as an Adequate Reperfusion Predictor in the Pharmaco-Invasive Approach
Henrique Tria Bianco
![]() , Rui Povoa
, Rui Povoa
![]() , Maria Cristina Izar
, Maria Cristina Izar
![]() , Braulio Luna Filho, Flavio Tocci Moreira, Edson Stefanini, Henrique Andrade Fonseca
, Braulio Luna Filho, Flavio Tocci Moreira, Edson Stefanini, Henrique Andrade Fonseca
![]() , Adriano Henrique Pereira Barbosa, Claudia Maria Rodrigues Alves, Adriano Mendes Caixeta, Iran Gonçalves Jr, Pedro Ivo de Marqui Moraes, Renato Delascio Lopes, Angelo Amato Vincenzo de Paola, Dirceu Almeida
, Adriano Henrique Pereira Barbosa, Claudia Maria Rodrigues Alves, Adriano Mendes Caixeta, Iran Gonçalves Jr, Pedro Ivo de Marqui Moraes, Renato Delascio Lopes, Angelo Amato Vincenzo de Paola, Dirceu Almeida
![]() , Valdir Ambrosio Moises, Francisco A. H. Fonseca
, Valdir Ambrosio Moises, Francisco A. H. Fonseca
![]()
This Original Article is referred by the Short Editorial "ST-Segment Elevation Regression as a Predictor of Reperfusion in Acute Myocardial Infarction: A Persistent Unknown".
Abstract
Background
Primary percutaneous coronary intervention is considered the “gold standard” for coronary reperfusion. However, when not available, the drug-invasive strategy is an alternative method and the electrocardiogram (ECG) has been used to identify reperfusion success.
Objectives
Our study aimed to assess ST-Segment changes in post-thrombolysis and their power to predict recanalization and using the angiographic scores TIMI-flow and Myocardial Blush Grade (MBG) as an ideal reperfusion criterion.
Methods
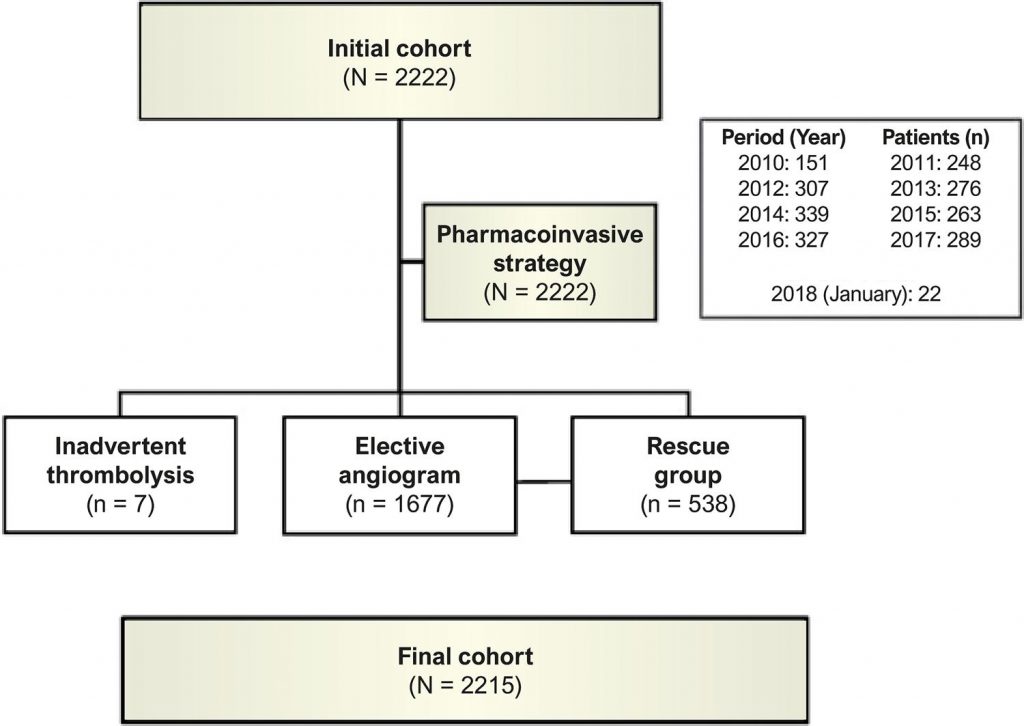
2,215 patients with ST-Segment Elevation Myocardial Infarction (STEMI) undergoing fibrinolysis [(Tenecteplase)-TNK] and referred to coronary angiography within 24 h post-fibrinolysis or immediately referred to rescue therapy were studied. The ECG was performed pre- and 60 min-post-TNK. The patients were categorized into 2 groups: those with ideal reperfusion (TIMI-3 and MBG-3) and those with inadequate reperfusion (TIMI and MBG <3). The ECG reperfusion criterion was defined by the reduction of the ST-Segment >50%. A p-value <0.05 was considered for the analyses, with bicaudal tests.
Results
The ECG reperfusion criterion showed a positive predictive value of 56%; negative predictive value of 66%; sensitivity of 79%; and specificity of 40%. There was a weak positive correlation between ST-Segment reduction and ideal reperfusion angiographic data (r = 0.21; p <0.001) and low diagnostic accuracy, with an AUC of 0.60 (95%CI: 0.57-0.62).
Conclusion
The ST-Segment reduction was not able to accurately identify patients with adequate angiographic reperfusion. Therefore, even patients with apparently successful reperfusion should be referred to angiography soon, to ensure adequate macro and microvascular coronary flow.
1,360