Arq. Bras. Cardiol. 2025; 122(5): e20240555
Acute Heart Failure in Patients with Chagas Cardiomyopathy: Results of the I Brazilian Heart Failure Registry (BREATHE)
Pedro Gabriel Melo de Barros e Silva
![]() , Denilson Campos Albuquerque
, Denilson Campos Albuquerque
![]() , Renato Delascio Lopes, Paulo Roberto Nogueira, Aguinaldo F Freitas Jr
, Renato Delascio Lopes, Paulo Roberto Nogueira, Aguinaldo F Freitas Jr
![]() , Carlos Vieira Nascimento, Charles Mady
, Carlos Vieira Nascimento, Charles Mady
![]() , Elizabete Silva dos Santos, Mauro Esteves Hernandes, Maria Alayde Mendonça Rivera
, Elizabete Silva dos Santos, Mauro Esteves Hernandes, Maria Alayde Mendonça Rivera
![]() , João David de Souza Neto, Alvaro Rabelo, Manoel Fernandes Canesin, Helder Reis, Anderson da Costa Armstrong, Conrado Hoffmann, Renato Hideo Nakagawa Santos, Isabella de Andrade Jesuino, Luis Eduardo Rohde
, João David de Souza Neto, Alvaro Rabelo, Manoel Fernandes Canesin, Helder Reis, Anderson da Costa Armstrong, Conrado Hoffmann, Renato Hideo Nakagawa Santos, Isabella de Andrade Jesuino, Luis Eduardo Rohde
![]() , Lidia Zytinsky Moura, Fabiana Goulart Marcondes-Braga, Evandro Tinoco Mesquita
, Lidia Zytinsky Moura, Fabiana Goulart Marcondes-Braga, Evandro Tinoco Mesquita
![]() , José Albuquerque de Figueiredo Neto
, José Albuquerque de Figueiredo Neto
![]() , Ricardo Mourilhe-Rocha
, Ricardo Mourilhe-Rocha
![]() , Luís Beck-da-Silva
, Luís Beck-da-Silva
![]() , Mucio Tavares Oliveira Junior
, Mucio Tavares Oliveira Junior
![]() , Marcus Vinicius Simões
, Marcus Vinicius Simões
![]()
This Original Article is referred by the Short Editorial "Acute Heart Failure Due to Chagas Disease: Still a Challenge in the 21st Century".
Abstract
Background
Although the clinical features of chronic Chagas’ cardiomyopathy (CCC) have been well established, clinical data about the patients are scarce.
Objectives
The current analysis reports the results of the I Brazilian Heart Failure Registry (BREATHE) assessing baseline characteristics and clinical outcomes of patients with acute heart failure due to CCC.
Methods
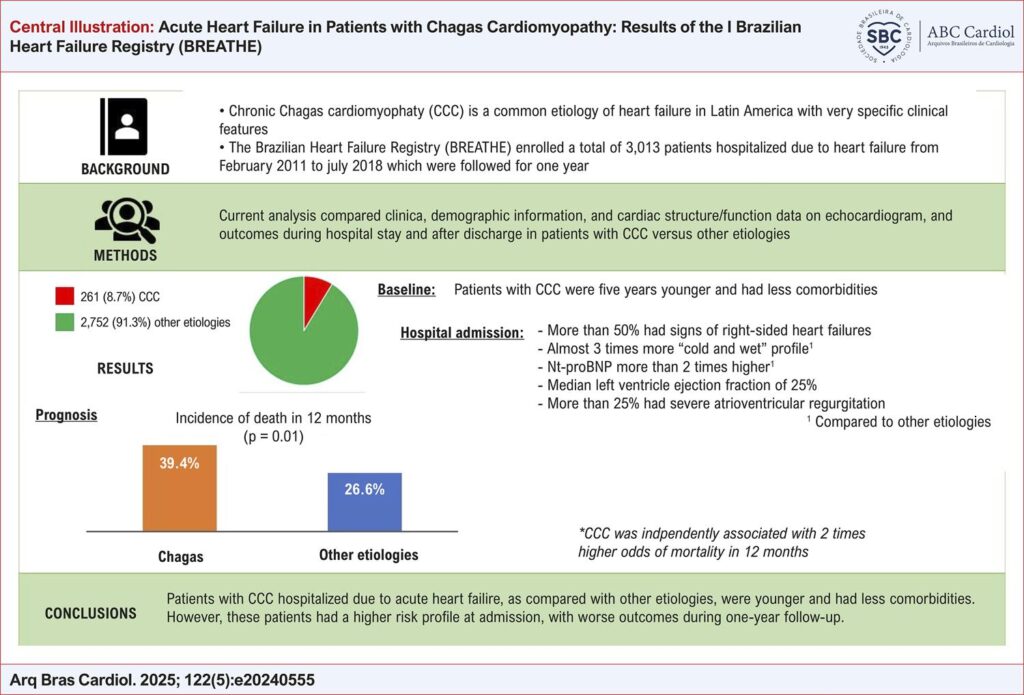
BREATHE enrolled a total of 3,013 adult patients hospitalized with acute heart failure. We analyzed comparatively 261 (8.7%) patients with chronic CCC and 2,752 (91.3%) patients with other etiologies. Clinical and demographic information, cardiac structure/function data on echocardiogram and outcomes during the hospital stay and after discharge were assessed in both groups. Uni and multivariate tests were performed and a p-value <0.05 was considered statistically significant.
Results
Patients with CCC presented lower systolic blood pressure (108.3 ± 26.1 vs 128.3 ± 30.3 mmHg, p<0.001) and left ventricle ejection fraction (25.4 [19 - 36]% vs 37 [27 - 54] %, p<0.001) with higher rates of jugular vein distension (54.8% vs 38.9%, p<0.001), hepatomegaly (47.9% vs 25.6%, p<0.001), and “cold and wet” clinical hemodynamic profile (27.2% vs 10.6%, p<0.001). Patients with CCC presented higher rate of the composite death or heart transplantation (17.4% vs. 11.1%, p=0.004), and higher cumulative incidence of death after 3 months (16.5% vs 10.8%, p=0.017), 6 months (25.3% vs 17.2%, p=0.006), and 12 months (39.4% vs 26.6%, p<0.001). Besides, CCC was independently associated with 12-month mortality risk with odds ratio = 2.02 (95% IC: 1.47-2.77).
Conclusion
Patients with CCC, hospitalized due to acute heart failure, in comparison to other etiologies, presented a higher risk profile that was associated with a poorer outcome during hospital stay and after discharge.
585