Arq. Bras. Cardiol. 2024; 121(4): e20230060
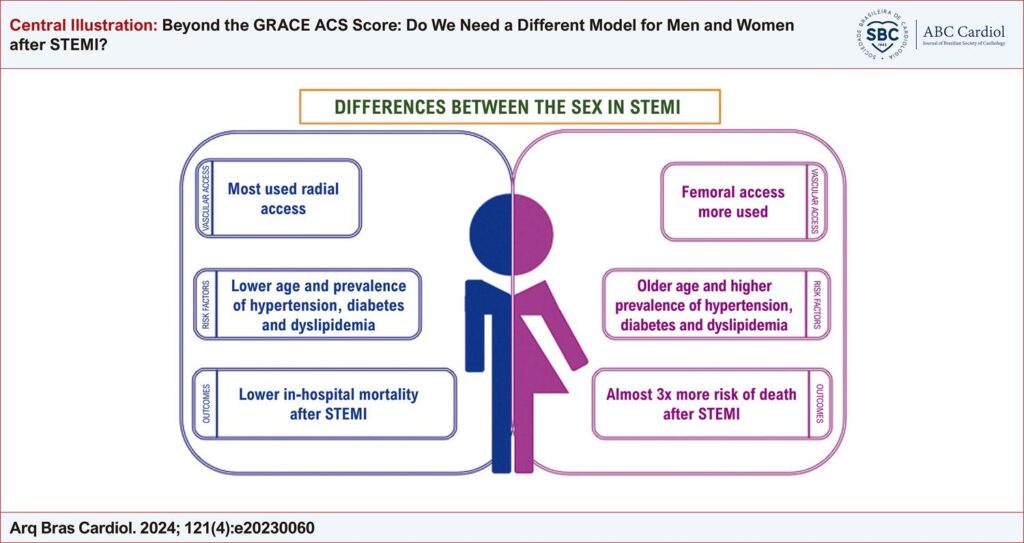
Beyond the GRACE ACS Score: Do We Need a Different Model for Men and Women after STEMI?
José Sergio Nascimento Silva
![]() , Isly Maria Lucena de Barros
, Isly Maria Lucena de Barros
![]() , Jorge Augusto Nunes Guimarães
, Jorge Augusto Nunes Guimarães
![]() , Davide Cao, Sílvia Marinho Martins
, Davide Cao, Sílvia Marinho Martins
![]() , Tawanna Xavier Marques de Carvalho, Rayssa Santana de Farias, Viviana Lemke
, Tawanna Xavier Marques de Carvalho, Rayssa Santana de Farias, Viviana Lemke
![]() , Roxana Mehran, Rodrigo Pedrosa
, Roxana Mehran, Rodrigo Pedrosa
![]()
This Original Article is referred by the Short Editorial "Can Artificial Intelligence Change our Interpretation of Cardiovascular Risk Scores?".
Abstract
Background
Women, in comparison to men, experience worse outcomes after acute coronary syndrome (ACS). However, whether the female sex per se is an independent predictor of such adverse events remains unclear.
Objective
This study aims to assess the association between the female sex and in-hospital mortality after ST-elevation myocardial infarction (STEMI).
Methods
We conducted a retrospective cohort study by enrolling consecutive STEMI patients admitted to a tertiary hospital from January 2018 to February 2019. All patients were treated per current guideline recommendations. Multivariable logistic regression models were applied to evaluate in-hospital mortality using GRACE variables. Model accuracy was evaluated using c-index. A p-value < 0.05 was statistically significant.
Results
Out of the 1678 ACS patients, 709 presented with STEMI. The population consisted of 36% women, and the median age was 61 years. Women were older (63.13 years vs. 60.53 years, p = 0.011); more often presented with hypertension (75.1% vs. 62.4%, p = 0.001), diabetes (42.2% vs. 27.8%, p < 0.001), and hyperlipidemia (34.1% vs. 23.9%, p = 0.004); and were less likely to undergo percutaneous coronary intervention (PCI) via radial access (23.7% vs. 46.1%, p < 0.001). In-hospital mortality rate was significantly higher in women (13.2% vs. 5.6%, p = 0.001), and the female sex remained at higher risk for in-hospital mortality (OR 2.79, 95% CI 1.15–6.76, p = 0.023). A multivariate model including age, sex, systolic blood pressure, cardiac arrest, and Killip class was 94.1% accurate in predicting in-hospital mortality, and the c-index was 0.85 (95% CI 0.77–0.93).
Conclusion
After adjusting for the risk factors in the GRACE prediction model, women remain at higher risk for in-hospital mortality.
1,607