Arq. Bras. Cardiol. 2021; 116(1): 119-126
Catheter Ablation of Focal Atrial Tachycardia with Early Activation Close to the His-Bundle from the Non Coronary Aortic Cusp
Muhieddine Chokr
![]() , Lucas G. de Moura
, Lucas G. de Moura
![]() , Italo Bruno dos Santos Sousa, Cristiano Faria Pisani
, Italo Bruno dos Santos Sousa, Cristiano Faria Pisani
![]() , Carina Abigail Hardy, Sissy Lara de Melo
, Carina Abigail Hardy, Sissy Lara de Melo
![]() , Arnobio Dias da Ponte Filho
, Arnobio Dias da Ponte Filho
![]() , Ieda Prata Costa
, Ieda Prata Costa
![]() , Ronaldo Vasconcelos Tavora, Luciana Sacilotto
, Ronaldo Vasconcelos Tavora, Luciana Sacilotto
![]() , Tan Chen Wu
, Tan Chen Wu
![]() , Francisco Carlos da Costa Darrieux, Denise Tessariol Hachul, Vera Demarchi Aiello
, Francisco Carlos da Costa Darrieux, Denise Tessariol Hachul, Vera Demarchi Aiello
![]() , Mauricio Scanavacca
, Mauricio Scanavacca
![]()
This Original Article is referred by the Short Editorial "Para-Hisian Atrial Tachycardia and Atrioventricular Nodal Reentry Tachycardia: After 25 Years The Same History?".
Abstract
Background
Atrial tachycardia (AT) ablation with earliest activation site close to the His-Bundle is a challenge due to the risk of complete AV block by its proximity to His-Purkinje system (HPS). An alternative to minimize this risk is to position the catheter on the non-coronary cusp (NCC), which is anatomically contiguous to the para-Hisian region.
Objectives
The aim of this study was to perform a literature review and evaluate the electrophysiological characteristics, safety, and success rate of catheter-based radiofrequency (RF) delivery in the NCC for the treatment of para-Hisian AT in a case series.
Methods
This study performed a retrospective evaluation of ten patients (Age: 36±10 y-o) who had been referred for SVT ablation and presented a diagnosis of para-Hisian focal AT confirmed by classical electrophysiological maneuvers. For statistical analysis, a p-value of <0.05 was considered statistically significant.
Results
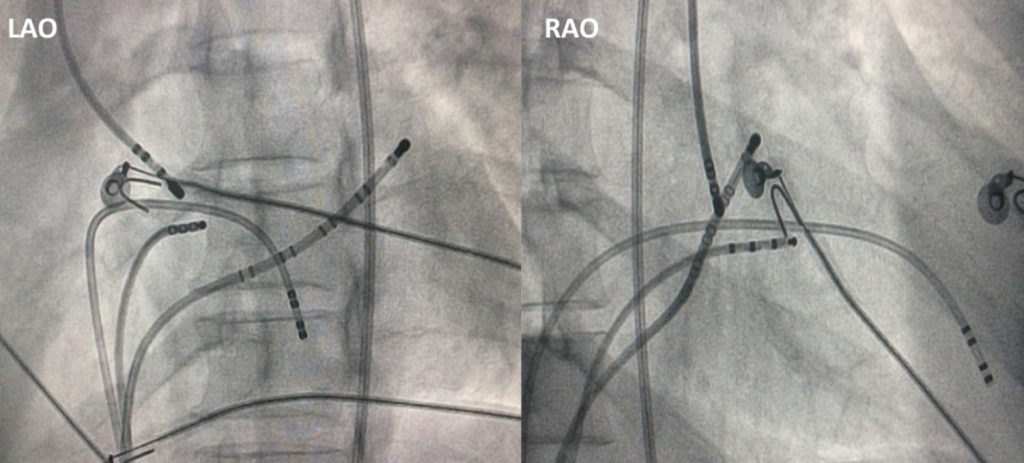
The earliest atrial activation at the His position was 28±12ms from the P wave and at the NCC was 3±2ms earlier than His position, without evidence of His potential in all patients. RF was applied on the NCC (4-mm-tip catheter; 30W, 55ºC), and the tachycardia was interrupted in 5±3s with no increase in the PR interval or evidence of junctional rhythm. Electrophysiological tests did not reinduce tachycardia in 9/10 of patients. There were no complications in all procedures. During the 30 ± 12 months follow-up, no patient presented tachycardia recurrence.
Conclusion
The percutaneous treatment of para-Hisian AT through the NCC is an effective and safe strategy, which represents an interesting option for the treatment of this complex arrhythmia. (Arq Bras Cardiol. 2021; 116(1):119-126)
1,606