Arq. Bras. Cardiol. 2022; 119(5): 778-788
F Wave Amplitude as a Predictor of Thromboembolism and Success of Electrical Cardioversion in Patients with Persistent Atrial Fibrillation
Renan Teixeira Campelo
![]() , Luciana Armaganijan, Dalmo A. R. Moreira, Matheus Kiszka Scheffer, Guilherme Dagostin de Carvalho
, Luciana Armaganijan, Dalmo A. R. Moreira, Matheus Kiszka Scheffer, Guilherme Dagostin de Carvalho
![]() , João Italo Dias França
, João Italo Dias França
![]()
This Original Article is referred by the Short Editorial "Fibrillatory Wave Amplitude: Should We Use It Routinely in Clinical Practice?".
Abstract
Background
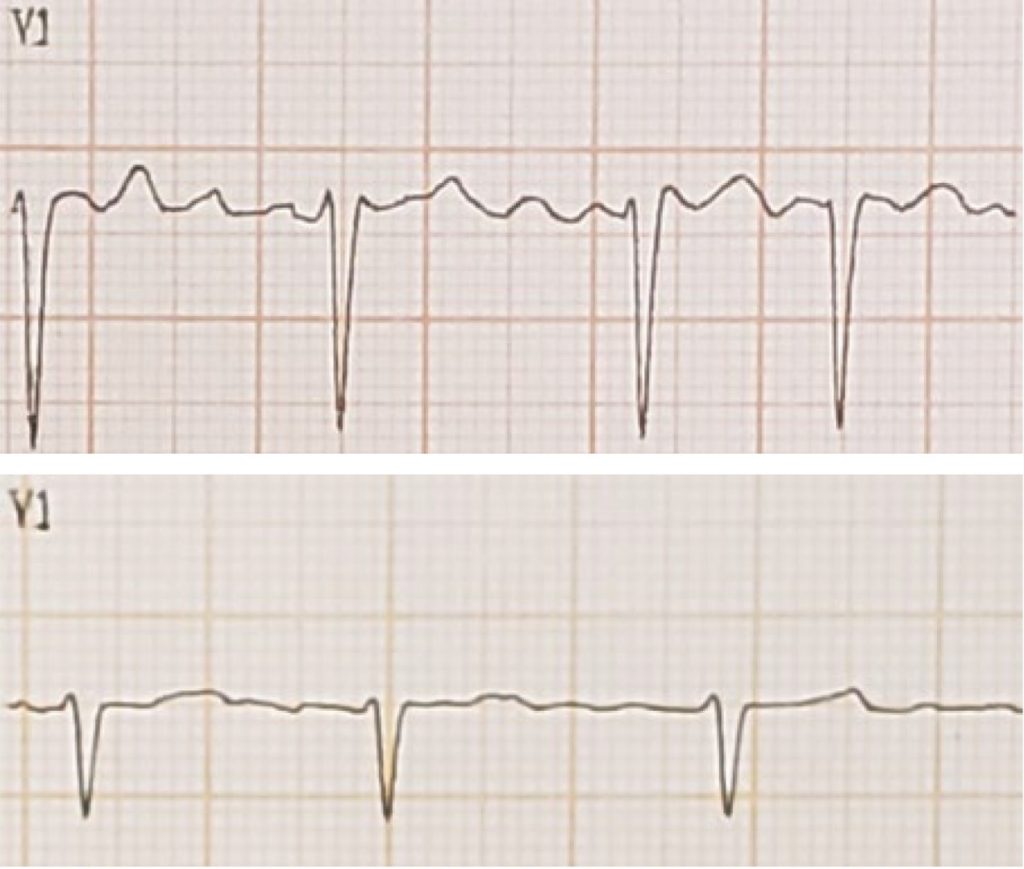
Atrial fibrillation (AF) is classified according to the amplitude of fibrillatory waves (f) into fine waves (fAF) and coarse waves (cAF).
Objectives
To correlate the amplitude of f waves with clinical, laboratory, electrocardiographic, and echocardiographic variables that indicate a high risk of thromboembolism and to assess their impact on the success of electrical cardioversion (ECV).
Methods
Retrospective, observational study that included 57 patients with persistent non-valvular AF who underwent ECV. The maximum amplitude of f waves was measured in lead V1. cAF was defined when f ≥ 1.0mm and fAF when f < 1.0mm. The findings were correlated with the indicated variables. Values of p < 0.05 were considered statistically significant.
Results
cAF (n = 35) was associated with greater success in ECV (94.3% vs. 72.7%, p = 0.036) even after adjusting for variables such as age and BMI (p = 0.026, OR = 11.8). Patients with fAF (n = 22) required more shocks and more energy to revert to sinus rhythm (p = 0.019 and p = 0.027, respectively). There was no significant association between f-wave amplitude and clinical, echocardiographic, and laboratory parameters.
Conclusions
The amplitude of f wave was not associated with echocardiographic, clinical and laboratory parameters that indicate a high risk of thromboembolism. cAF was associated with a higher chance of success reverting to sinus rhythm employing ECV. A greater number of shocks and energy were required for reversion to sinus rhythm in patients with fAF.
937