Arq. Bras. Cardiol. 2022; 119(6): 996-998
Left Ventricular Thrombosis and Pulmonary Thromboembolism in an Asymptomatic Covid-19 Patient
Natalia Lorenzo
![]() , Veronica Hernandez, Alvaro Montes, Fernando Rivero, Guillermo Reyes*, Rio Aguilar
, Veronica Hernandez, Alvaro Montes, Fernando Rivero, Guillermo Reyes*, Rio Aguilar
![]()
Research Letter
A 48-year-old-man presented to the emergency room with abdominal pain and vomiting of 12-hour duration. He had a history of porto-splenic venous thrombosis ten years before admission that was treated with 6 months of oral anticoagulation and felt to be due to moderate protein C deficiency, which was not confirmed in subsequent laboratory tests. Vital signs were normal, he was afebrile and no remarkable findings were found on physical examination except for pain on palpation in the left flank. The reverse transcriptase polymerase chain reaction (RT-PCR) test for COVID-19 was negative. Blood tests showed significant elevation of acute phase reactants (c-reactive protein: 138.3 mg/L, fibrinogen > 500mg/dL and leukocites 12.99 10^3/μL). Coagulation parameters where in normal range: phrotrombin time (PT) 12.1 seconds, partial thromboplastin time (PTT) 36.3 seconds, prothrombin activity (PA) 86%, international normalized ratio (INR) 1.08 and platelets 326.000/μL.
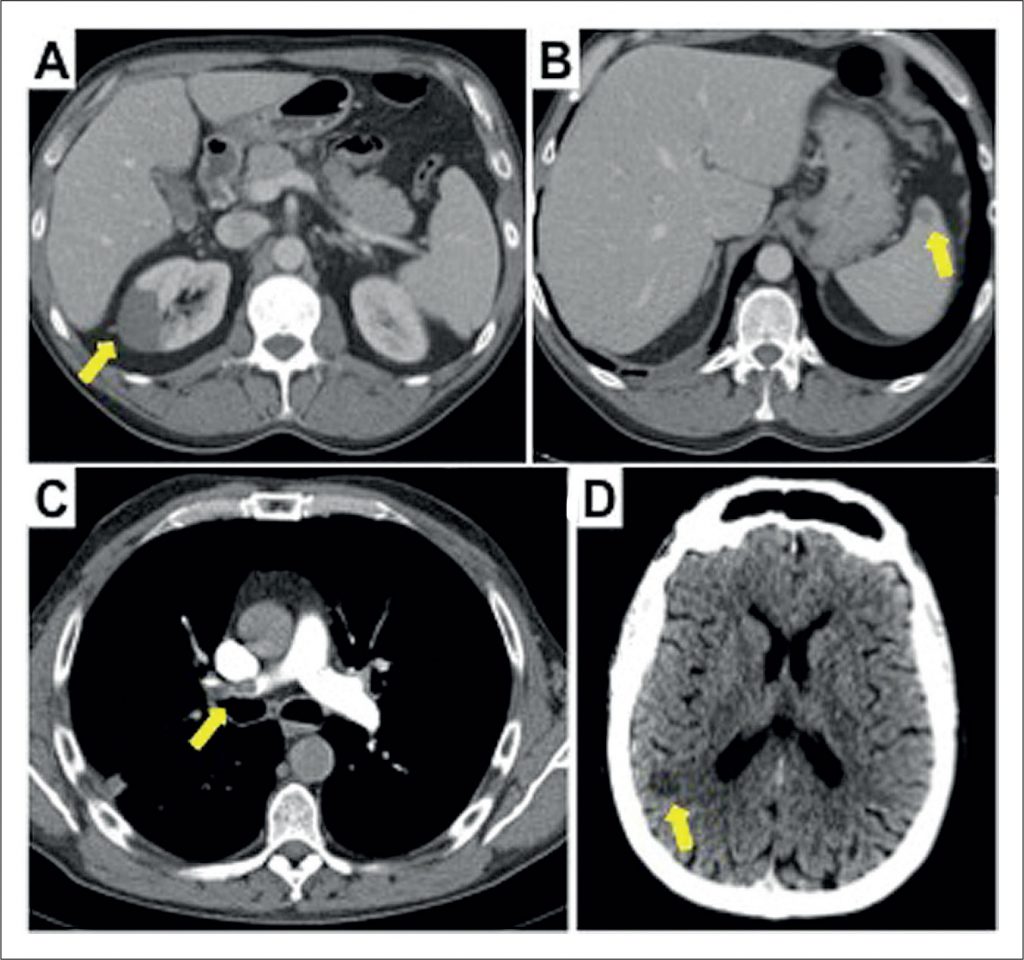
The abdominal ultrasound-scan did not show releant findings, so a computed tomography (CT) scan study was completed. CT abdominal scan found multiple infarcts in the right kidney () and isolated in spleen (), furthermore, a filling defect in the left ventricle was observed (). Transthoracic echocardiogram confirmed the presence of a pedunculated hyperechogenic and homogeneous mobile mass (3.1x2cm) with regular borders (, , ), anchored to the middle third of the septum of left ventricle (LV). Anatomy of LV was normal, with normal dimensions and normal ejection fraction without wall motion abnormalities.
[…]
1,200