Arq. Bras. Cardiol. 2022; 119(5): 809-812
Mitral Valve Perforated Aneurysm: An Issue of Inflammation or Pressure Gradients?
Inês Oliveira
![]() , Isabel Cruz, Ana Neto
, Isabel Cruz, Ana Neto
![]() , Bruno Bragança
, Bruno Bragança
![]() , Glória Abreu, João Azevedo, Aurora Andrade
, Glória Abreu, João Azevedo, Aurora Andrade
Case Report
Mitral valve aneurysms (MVA) are uncommon and usually develop acutely in the setting of infective endocarditis (IE). MVA as a late complication of IE in a patient with obstructive hypertrophic cardiomyopathy (HCM) is rather unusual, raising considerations regarding the role of the infectious process and the hemodynamic conditions inherent to the cardiomyopathy. , We present a case report of a patient with HCM and a ruptured aneurysm of the mitral valve (MV) leaflet, secondary to previously treated IE.
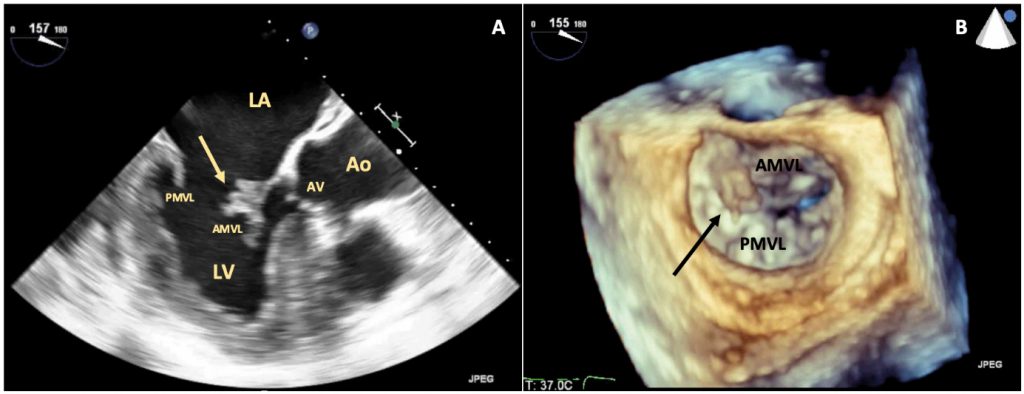
A 68-year-old male patient with type 2 diabetes mellitus and dyslipidemia was admitted to a hospital with a 3-week history of malaise, fever, and recent left-sided abdominal pain. His physical examination revealed a grade II/VI systolic heart murmur at the cardiac apex, fever, abdominal tenderness in the left upper quadrant, and purpuric lesions in the inferior limbs. Blood analyses showed neutrophilia and C-Reactive Protein of 211mg/L. Positive blood cultures indicated Staphylococcus aureus methicillin-sensitive. Abdominal Computed Tomography revealed spleen embolization, with no abscess. Transthoracic (TTE) and transesophageal echocardiography (TEE) disclosed a highly mobile polypoid mass in the atrial side of the anterior MV leaflet, suggestive of a vegetation, with mild mitral regurgitation and no evidence of abscess, aneurysm, or valve perforation; asymmetrical left ventricular (LV) hypertrophy with the presence of an increased intraventricular systolic gradient (IVSG) and systolic anterior motion (SAM) of the MV ( ). The diagnosis of IE in HCM was established and treated accordingly with flucloxacillin, presenting a favorable clinical evolution. After three months of follow-up, cardiac magnetic resonance was performed, confirming the diagnosis of HCM: an increased LV mass (96g/m ) with asymmetrical left ventricular hypertrophy (maximal thickness of 20mm in the inferoseptal wall), with no perfusion defects but with evidence of intramural late gadolinium enhancement in the inferoseptal wall,and SAM of the MV ( ). Echocardiography was repeated and, in addition to evidence of obstructive HCM with a rest IVSG of 44 mmHg, an aneurysm of the anterior leaflet of the MV was identified. Two mitral regurgitant jets were observed, one due to incomplete coaptation of the leaflets and another through the perforated aneurysm, quantifying global mitral regurgitation (MR) in a moderate (grade II/IV) ( ). The beta-blocker dose was increased, and a strategy of close follow-up was adopted. Maintenance of the characteristics of the aneurysm was verified in outpatient follow-up after 2 years.
[…]
1,324