Arq. Bras. Cardiol. 2020; 115(5): 964-966
Non-Progressive Hepatic Form of Andersen Disease as a Mimic of Hypertrophic Cardiomyopathy
Fabio Mastrocola, William Santos de Oliveira
![]() , Adalberto Atsushi Porto, Roberto Moreno Mendonça, Nestor Rodrigues de Oliveira Neto
, Adalberto Atsushi Porto, Roberto Moreno Mendonça, Nestor Rodrigues de Oliveira Neto
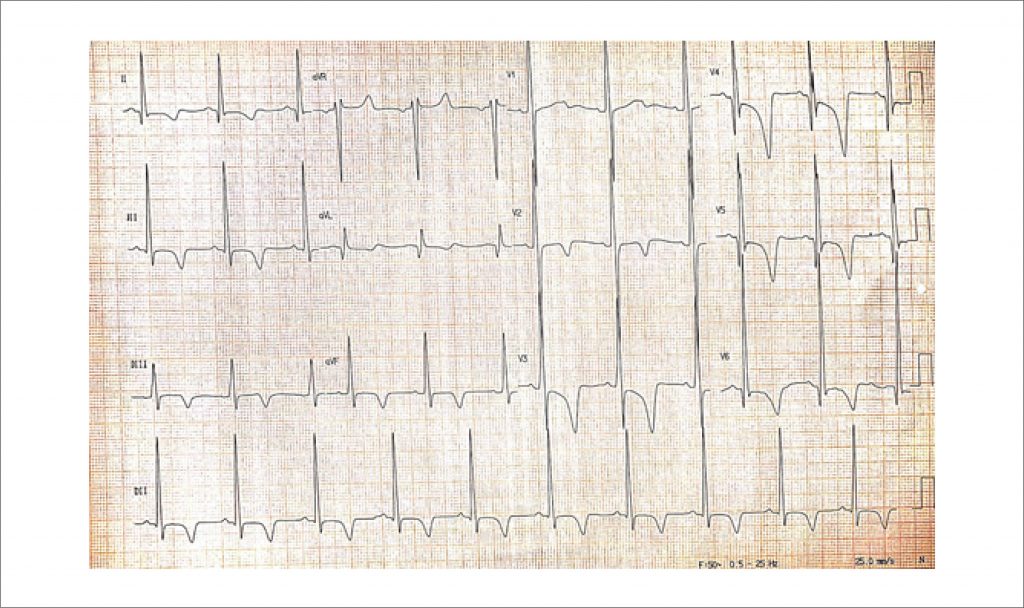
An 18-year-old male patient presented to our ambulatory services due to a 3-month course of progressive dyspnea and non-productive cough. Symptoms were present even at rest, and he exhibited severe limitation at physical activity. He had a diagnosis of glycogen storage disease (GSD) type IV attained by liver biopsy since three years of age, when he developed hepatomegaly and mild hepatic dysfunction. At the time, histopathological examination showed grade 2 fibrosis along with numerous intracytoplasmic PAS-positive deposits that were resistant to diastase. Thenceforth, his liver function remained stable, and he persisted otherwise asymptomatic. His physical examination was unremarkable, and routine laboratory evaluation was within the normal ranges. However, his basal ECG () showed signs of left ventricular hypertrophy. He was submitted to a cardiovascular magnetic resonance (CMR), which showed asymmetrical hypertrophy with predominance in the interventricular septum (). Late gadolinium enhancement (LGE) was present in a patchy, multifocal pattern (). Medical therapy for heart failure was initiated; the patient is now asymptomatic and maintains regular follow-up in our ambulatory.
Patients with classic GSD type IV have unrelenting liver disease with fast progression to cirrhosis during childhood; however, a small subset of affected individuals may present with milder hepatic dysfunction that does not advance to end-stage liver disease., Accordingly, our patient had the diagnosis of GSD type IV by three years of age, but did not develop cirrhosis afterwards.
[…]
730