Arq. Bras. Cardiol. 2021; 116(5): 1023-1026
Prosthetic Aortic Valve Endocarditis by Neisseria Elongata after Bentall Procedure: When Multimodality Imaging is Key to Diagnosis
Mariana Brandão
![]() , Pedro Gonçalves-Teixeira
, Pedro Gonçalves-Teixeira
![]() , Pedro Ribeiro Queirós, Nuno Dias Ferreira, Marco Oliveira
, Pedro Ribeiro Queirós, Nuno Dias Ferreira, Marco Oliveira
A diabetic 65-year-old male with previous Bentall procedure and mechanical aortic valve prosthesis presented with fever and abdominal pain, along with systolic murmur (III/VI) and elevated inflammatory markers. Abdominal computed tomography (CT) revealed splenic infarction. Transesophageal echocardiogram (TEE) was negative for vegetations. Given the persistent suspicion of infective endocarditis (IE) with peripheral embolism, empirical antimicrobial therapy was initiated. The patient subsequently presented with complete atrioventricular block, requiring temporary transvenous pacing. An epicardial pacemaker was later implanted.
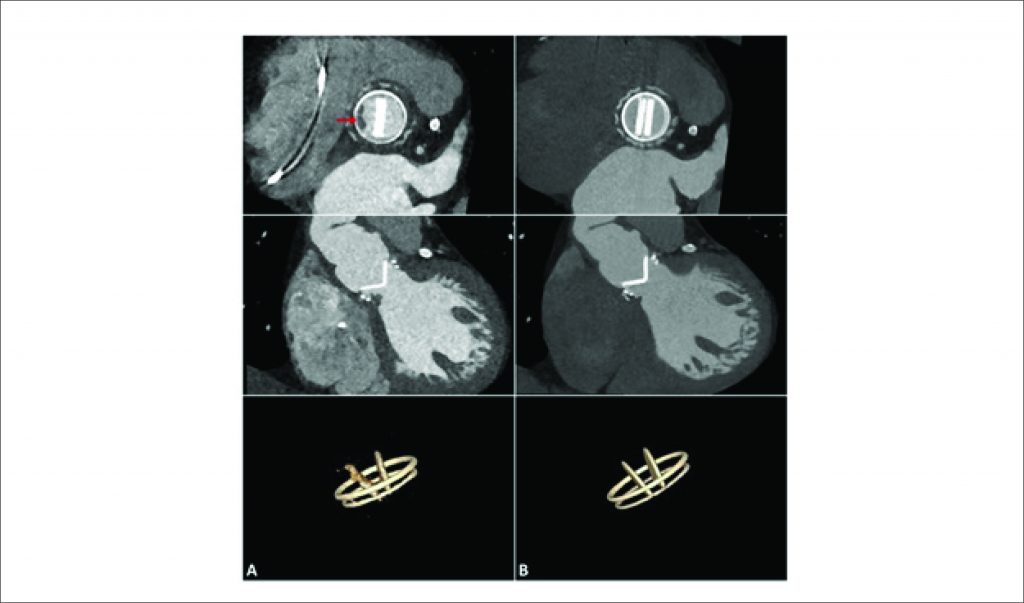
At the time, cardiac CT revealed an irregular-shaped hypoattenuating mass attached to the ventricular side of the prosthetic suture ring, consistent with vegetation (), interfering with the normal opening of one of the prosthesis discs (). Repeat TEE also showed a small highly mobile vegetation and an annular abscess in the prosthetic aortic valve (). Blood cultures were positive for Neisseria elongata, confirming the diagnosis of prosthetic valve endocarditis (PVE); antimicrobial therapy was tailored. Despite early improvement, the patient later presented with de novo ataxia and brain CT revealed infarction in the right vertebrobasilar territory. New sets of cultures remained negative and coagulation levels were within therapeutic range. A small vegetation persisted on cardiac CT and TEE, and inflammatory infiltrate was apparent at the mitro-aortic curtain.
[…]
975