Arq. Bras. Cardiol. 2024; 121(2): e20230350
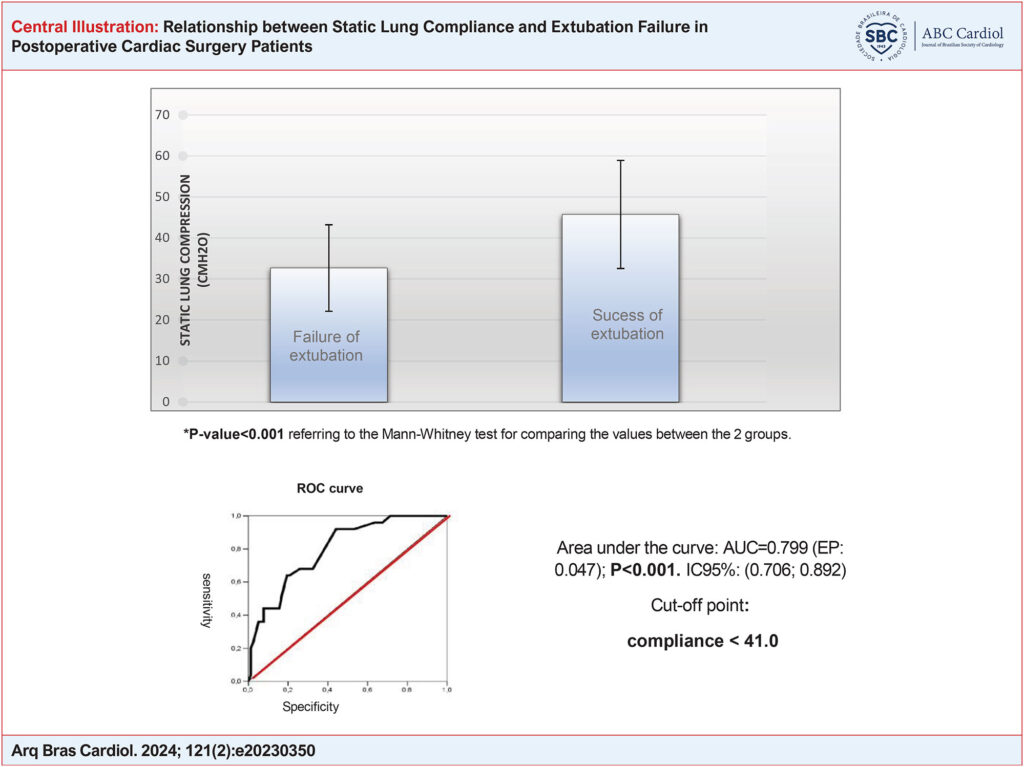
Relationship between Static Lung Compliance and Extubation Failure in Postoperative Cardiac Surgery Patients
Thais Bento Rudge Ramos
![]() , Luciana Castilho Figueiredo, Luiz Claudio Martins, Antonio Luis Eiras Falcão, Lígia dos Santos Roceto Ratti
, Luciana Castilho Figueiredo, Luiz Claudio Martins, Antonio Luis Eiras Falcão, Lígia dos Santos Roceto Ratti
![]() , Orlando Petrucci, Desanka Dragosavac
, Orlando Petrucci, Desanka Dragosavac
This Original Article is referred by the Short Editorial "Relationship between Static Lung Compliance and Extubation After Cardiac Surgery".
Introduction
Extubation failure is associated with higher morbidity and mortality, longer mechanical ventilation time, and delayed recovery, prolonging the patient’s hospital stay. Between 4% and 20% of extubated patients fail extubation, i.e., they are reintubated in the first 42 to 72 hours after extubation. According to studies, extubation failure in patients undergoing cardiac surgery can be predicted by several variables, such as the patient’s previous medical history, laboratory data, rapid shallow breathing index (RSBI), surgical variables such as the complexity and duration of the surgery and cardiopulmonary bypass (CPB) time., However, other potential predictors have not been adequately considered, and the protocols used to identify whether the patient is able to take up and maintain ventilation adequately are still general and not widely agreed upon.
Since the early 1990s, post-cardiac surgery patients have been extubated as soon as their hemodynamics, level of consciousness, and spontaneous ventilatory capacity are stabilized. The method known as “fast track” aims to reduce pulmonary complications linked to mechanical ventilation, speed up recovery, and reduce ICU stay and hospital costs. There is no consensus in the literature regarding the time for extubation; the period varies from two hours to twelve hours after the end of the surgery, while other studies advocate extubation while still in the operating room, which has become known as “ultra-fast-track”. Successful extubation is achieved by maintaining spontaneous ventilation for 48 hours after extubation.
[…]
Keywords: Lung Compliance; Postoperative Care; Thoracic Surgery
878