Arq. Bras. Cardiol. 2023; 120(1): e20220248
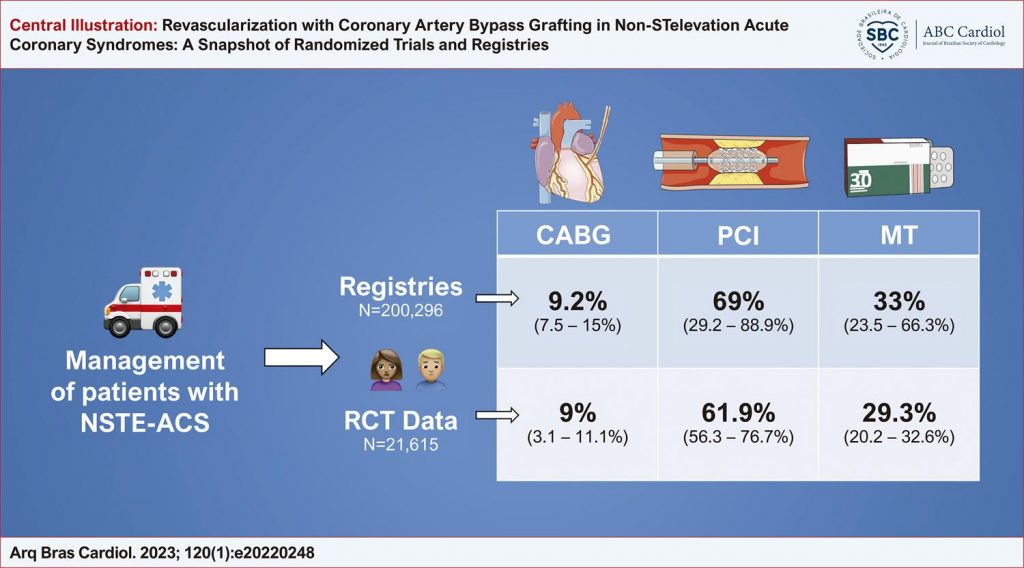
Revascularization with Coronary Artery Bypass Grafting in Non-ST-elevation Acute Coronary Syndromes: A Snapshot of Randomized Trials and Registries
Josip Andelo Borovac
![]() , Jerko Ferri-Certic, Dino Miric, Jaksa Zanchi, Mislav Lozo, Anteo Bradaric
, Jerko Ferri-Certic, Dino Miric, Jaksa Zanchi, Mislav Lozo, Anteo Bradaric
![]() , Konstantin Schwarz, Chun Shing Kwok
, Konstantin Schwarz, Chun Shing Kwok
![]()
A recent European Society of Cardiology (ESC) guidelines for the management of patients presenting with acute coronary syndromes (ACS) without persistent ST-segment elevation (NSTE-ACS) do not recommend routine pretreatment with a P2Y12 receptor antagonist in patients in which the coronary anatomy is undetermined, and early invasive management is planned (class recommendation III, level of evidence A). The rationale for such recommendation was mainly based on the results obtained from two large randomized trials, ACCOAST and ISAR-REACT 5, and analysis from the Swedish Coronary Angiography and Angioplasty Registry (SCAAR), showing that administration of P2Y12 inhibitor before the knowledge of coronary anatomy in patients with NSTE-ACS did not improve ischemic outcomes and significantly increased risk of bleeding.
Some of the clinical concerns associated with upstream platelet inhibition in NSTE-ACS are based on the notion that such a strategy might be harmful in patients with other conditions mimicking NSTE-ACS, such as aortic dissection or may be at risk for major or fatal bleeding events such as intracranial bleeding. Likewise, NSTE-ACS patients who would need to undergo coronary artery bypass graft (CABG) surgery after their coronary anatomy is visualized by diagnostic coronary angiography might be at increased risk of bleeding complications and procedural delays due to receipt of P2Y12 inhibitor pretreatment since 3 to 7 days are required to allow for recovery of platelet function prior to CABG. Furthermore, there are complex discretion factors in real-life, such as surgical hesitancy or decline to operate on a patient on a current dual antiplatelet treatment (DAPT). It should also be noted that non-CABG-related bleeding is a relevant concern for clinicians, such as gastrointestinal bleeding or catheterization access bleeding, and these complications are likely to be more frequent with pretreatment use. Since the latest ESC guidelines state that “pretreatment strategy might be harmful to a relevant proportion “of such patients, we sought to determine what exactly is the proportion of patients with NSTE-ACS that were referred to CABG surgery following angiography and we report on the prevalence of high-risk features that might predispose them to a potential receipt of surgical revascularization.
[…]
1,050