Arq. Bras. Cardiol. 2023; 120(10): e20230133
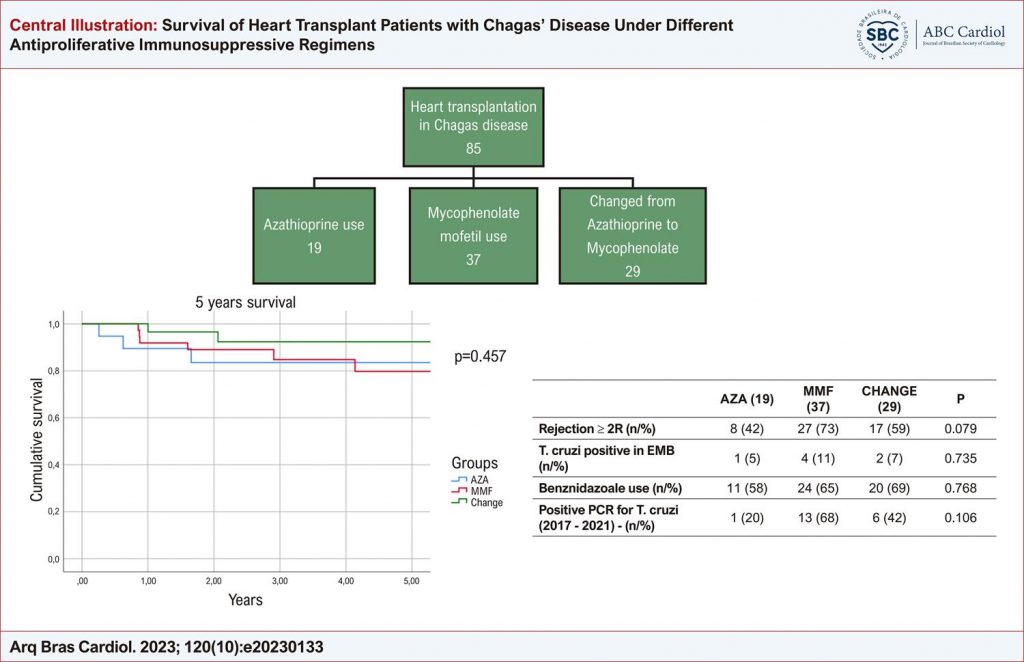
Survival of Heart Transplant Patients with Chagas’ Disease Under Different Antiproliferative Immunosuppressive Regimens
Silas Ramos Furquim
![]() , Luana Campoli Galbiati, Monica S. Avila
, Luana Campoli Galbiati, Monica S. Avila
![]() , Fabiana G. Marcondes-Braga
, Fabiana G. Marcondes-Braga
![]() , Julia Fukushima, Sandrigo Mangini, Luis Fernando Bernal da Costa Seguro, Iascara Wozniak de Campos, Tania Mara Varejão Strabelli, Fernanda Barone, Audrey Rose da Silveira Amancio de Paulo, Luciana Akutsu Ohe, Mariana Cappelletti Galante, Fabio Antonio Gaiotto, Fernando Bacal
, Julia Fukushima, Sandrigo Mangini, Luis Fernando Bernal da Costa Seguro, Iascara Wozniak de Campos, Tania Mara Varejão Strabelli, Fernanda Barone, Audrey Rose da Silveira Amancio de Paulo, Luciana Akutsu Ohe, Mariana Cappelletti Galante, Fabio Antonio Gaiotto, Fernando Bacal
Abstract
Background
Chagas’ disease (CD) is an important cause of heart transplantation (HT). The main obstacle is Chagas’ disease reactivation (CDR), usually associated to high doses of immunosuppressants. Previous studies have suggested an association of mycophenolate mofetil with increased CDR. However, mortality predictors are unknown.
Objectives
To identify mortality risk factors in heart transplant patients with CD and the impact of antiproliferative regimen on survival.
Methods
Retrospective study with CD patients who underwent HT between January 2004 and September 2020, under immunosuppression protocol that prioritized azathioprine and change to mycophenolate mofetil in case of rejection. We performed univariate regression to identify mortality predictors; and compared survival, rejection and evidence of CDR between who received azathioprine, mycophenolate mofetil and those who changed from azathioprine to mycophenolate mofetil after discharge (“Change” group). A p-value < 0.05 was considered statistically significant.
Results
Eighty-five patients were included, 54.1% men, median age 49 (39-57) years, and 91.8% were given priority in waiting list. Nineteen (22.4%) used azathioprine, 37 (43.5%) mycophenolate mofetil and 29 (34.1%) switched therapy; survival was not different between groups, 2.9 (1.6-5.0) x 2.9 (1.8-4.8) x 4.2 (2.0-5.0) years, respectively; p=0.4. There was no difference in rejection (42%, 73% and 59% respectively; p=0.08) or in CDR (T. cruzi positive by endomyocardial biopsy 5% x 11% x 7%; p=0.7; benznidazole use 58% x 65% x 69%; p=0.8; positive PCR for T. cruzi 20% x 68% x 42% respectively; p=0.1) rates.
Conclusions
This retrospective study did not show difference in survival in heart transplant patients with CD receiving different antiproliferative regimens. Mycophenolate mofetil was not associated with statistically higher rates of CDR or graft rejection in this cohort. New randomized clinical trials are necessary to address this issue.
Keywords: Chagas Disease; Heart Transplantation; Survival
914